Medical and surgical therapy . musclesthemselves do not contract. Their tendons, whichowing to the drooping position of the hand are veryapparent at the level of the wrist, never move at all. To verify abolition of lateral movements of the wTist,which are normally performed by the extensor carpiradialis longior and the extensor carpi ulnaris, possi-bilities of error arising from the movement of theelbow should be eliminated by resting the forearm ona table, as in examination for extension of the hand ;but the hand should be raised almost to the hori-zontal instead of being allowed to drop. Ind
{kind=link}
Image details
Contributor:
The Reading Room / Alamy Stock PhotoImage ID:
2AM4T6AFile size:
7.1 MB (549.4 KB Compressed download)Releases:
Model - no | Property - noDo I need a release?Dimensions:
2141 x 1167 px | 36.3 x 19.8 cm | 14.3 x 7.8 inches | 150dpiMore information:
This image is a public domain image, which means either that copyright has expired in the image or the copyright holder has waived their copyright. Alamy charges you a fee for access to the high resolution copy of the image.
This image could have imperfections as it’s either historical or reportage.
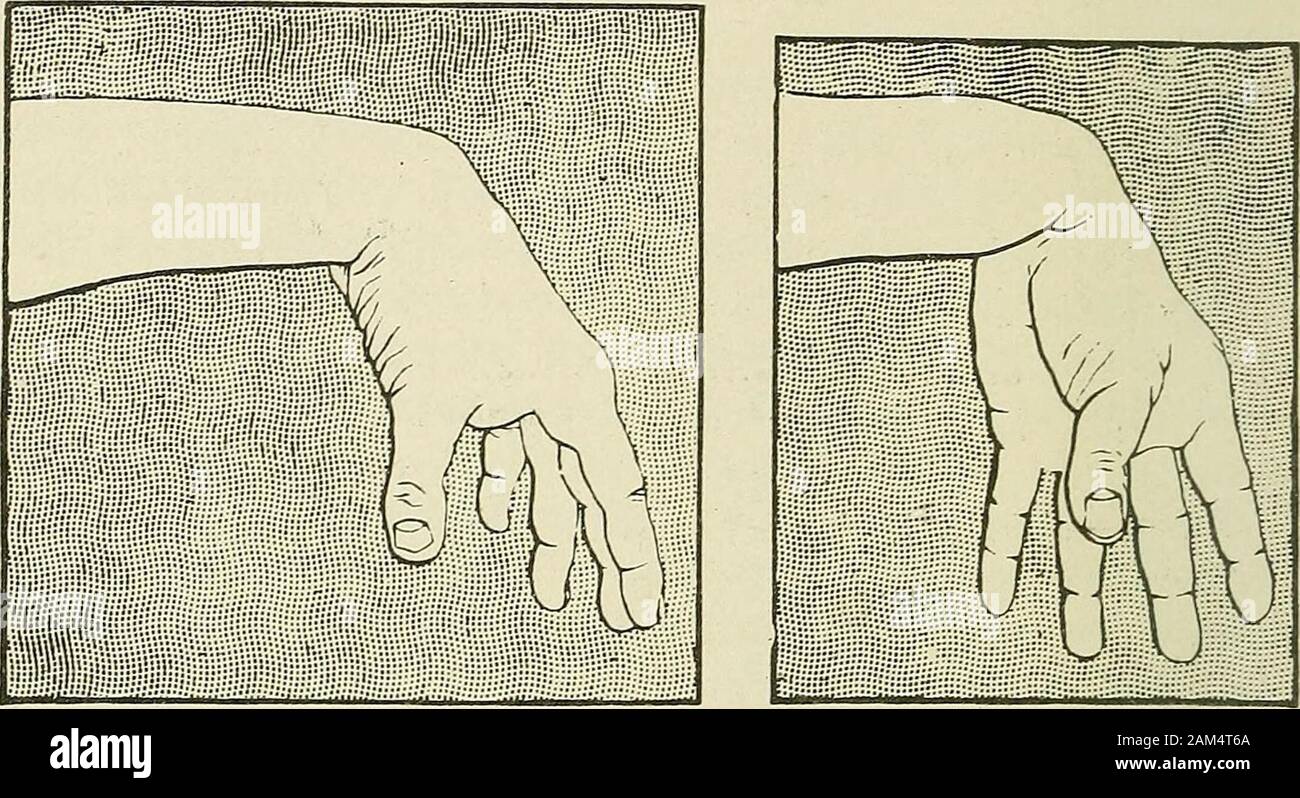
Medical and surgical therapy . musclesthemselves do not contract. Their tendons, whichowing to the drooping position of the hand are veryapparent at the level of the wrist, never move at all. To verify abolition of lateral movements of the wTist, which are normally performed by the extensor carpiradialis longior and the extensor carpi ulnaris, possi-bilities of error arising from the movement of theelbow should be eliminated by resting the forearm ona table, as in examination for extension of the hand ;but the hand should be raised almost to the hori-zontal instead of being allowed to drop. Indeed, 32 CLINICAL FORMS OF NERVE LESIONS Duchenne (of Boulogne) proved that, as the wristbends, lateral movements diminish.^ Extensors of the Fingers {Extensor communis digi-torum, extensor indicis, extensor minimi digiti).—Theextensors of the fingers extend the first phalanx ofthe fingers on the metacarpal bones, and only the firstphalanx. The extension of the second and thirdphalanges is performed by the interossei and the. Fig. 9.—Musculo-spiral paralysis. Pos-ture of hand in attempted extensionof the fingers. Slight extension of lasttwo phalanges can be carried out bythe assistance of the interossei: butthe first phalanx cannot be extendedon the metacarpus. Fig. 10.—Mitsculo-spiral par-alysis. Posture of handand fingers in attemptedabduction of the thumb. lumbricales. The slight degree of extension of thesetwo phalanges made by the patient in his efforts toextend the fingers on the metacarpus must not beattributed to restoration of the musculo-spiral nerve(fig. 9). To demonstrate the immobility of the first phalanx, the patients forearm should be rested on the table ^ The action of the flexor carpi radialis as an abductor muscle, andthat of the flexor carpi ulnaris as an adductor, is negligible. Duchennedenies that these muscles take part in any way in lateral movementsof the wrist. THE MUSCULO-SPIRAL NERVE 33 with the wrist semi-extended, and he should be askedto exten